Patellar tendinitis, also known as Jumper’s knee, is an overuse injury causing front knee pain, particularly at the base of the kneecap (patella).
Patellar tendonitis symptoms
Symptoms of Patellar tendinitis gradually manifest, including:
- Pain at the kneecap’s base
- Pain during quadriceps contraction or squatting
- Post-exercise aching and stiffness
- Occasional acute pain flares
- Tenderness upon pressing the kneecap’s base
- Thickened affected tendon
Notably, the condition, termed Jumper’s knee, inflicts significant discomfort during jumping activities.
How bad is my Jumper’s Knee?
Jumper’s knee injuries are classified into grades 1 through 4, based on pain severity.
Jumper’s Knee Grades:
- Pain post-training.
- Pain pre and post-training eases upon warming up.
- Pain during training, hampers performance.
- Pain during everyday activities.
Additional symptoms might include a weakened or atrophied vastus medialis oblique (VMO) muscle inside the thigh and calf muscle weakness.
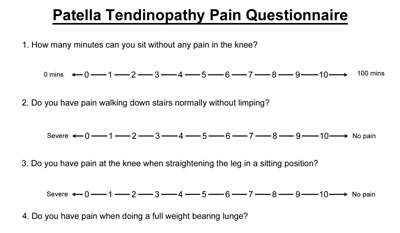
VISA pain questionnaire for Patellar tendonitis
The VISA pain questionnaire, ideal for monitoring hard-to-describe chronic condition symptoms, helps track progress. A lower score indicates a more severe injury. We recommend weekly check-ins.
What is Patellar tendonitis?
Patella tendinitis refers to the inflammation of the patella tendon, located at the front of the knee. In chronic cases, the condition often involves more degeneration than inflammation, thus “patella tendinopathy” may be a more accurate term. Throughout this article, both terms are used interchangeably.
The patella tendon, also known as the patella ligament, is remarkably strong. It connects the kneecap, or patella, to the shin bone, also known as the tibia. The powerful quadriceps muscles at the front of the thigh exert significant forces on the kneecap, especially during jumping and landing, thereby stressing the patella tendon.
What causes Jumper’s knee/Patella tendonitis?
Jumper’s knee, or patellar tendinopathy, is an overuse injury often associated with chronic tendon degeneration. While acute inflammation tends to subside with short rest, the condition is characterized by micro-tears and collagen degeneration in the tendon. Risks can be heightened by factors such as improper foot biomechanics, weak quadriceps muscles, and incorrect training techniques.
Q angle of the knee & VMO
The Q angle of the knee indicates the orientation of the femur (thigh bone) to the tibia (shin bone). Athletes suffering from patella tendinitis frequently exhibit the impaired function of the Vastus medialis obliquus (VMO)—the inner quadriceps muscle near the knee—and significant calf muscle weakness.
Patellar tendonitis treatment
Patellar tendinitis treatment aims to alleviate pain, stretch the quadriceps muscles, and gradually amplify the load borne by your knee.
Cold therapy
Implement the PRICE principles: Protection, Rest, Ice, Compression, and Elevation. Regularly apply cold therapy, particularly in the initial 24 to 48 hours and post-exercise. Use a cold therapy wrap or gel ice pack. If experiencing pain, apply ice for 10 minutes every hour, decreasing frequency as symptoms improve.
Warning: Underestimating jumper’s knee can lead to serious consequences. Athletes might be tempted to continue training and competing, but a seemingly quick recovery can be misleading. Neglecting this injury could result in a chronic condition, necessitating extensive treatment and possibly even surgery. Please proceed with caution.
Jumpers knee taping
Patella taping is a straightforward technique to alleviate patella tendinitis symptoms. It modifies the force direction through the tendon. Compressing the patella tendon beneath the knee changes the tendon’s pull angle on the patella, thus reducing strain on the affected area.
Patella tendonitis strap
Consider wearing a knee support or jumper’s knee strap to mitigate pain and relieve tendon strain. A jumper’s knee strap, wrapped around your knee, over the tendon, and just below the patella, alters the tendon’s angle against the patella. Consequently, it adjusts the area of the tendon that absorbs the force.
Medication
A doctor might recommend anti-inflammatory medication such as ibuprofen. Always consult a doctor before taking any medication and avoid ibuprofen if you have asthma. While such medication may temporarily alleviate acute inflammation and pain, it could potentially impede later healing.
Electrotherapy
A professional therapist might employ electrotherapy, using ultrasound or laser treatment, to decrease pain, reduce inflammation, and facilitate healing.
Massage
Cross-friction massage for patellar tendinitis applies deep, transverse pressure across the tendon. Suitable for chronic cases, this technique aids in realigning new fibres and could stimulate healing by prompting an acute response. Thigh massage can also help relax the muscles, augmenting the efficacy of stretching exercises.
Injections
Aprotinin injections may aid tendinopathies by rebalancing tendon enzymes. If conservative treatments prove ineffective, surgery could be necessary.
Surgery for Patellar tendonitis
The surgical approach to treating jumper’s knee varies depending on the individual case and the surgeon’s preference. The procedure carries a success rate of around 60-80%. Post-surgery, a full return to previous sports levels may take 6 to 12 months, and while many attain this, some may not. Surgery is typically considered only after exhausting conservative treatment methods.
The procedure commonly involves a longitudinal or transverse incision over the patella tendon, followed by the removal of abnormal tissue. Surgeons may opt for a longitudinal or transverse cut into the tendon, or for arthroscopy (keyhole surgery) versus open surgery.